 University Journal of Surgery and Surgical Specialities
University Journal of Surgery and Surgical Specialities
Intestinal Neuroendocrine Tumour Presenting as Acute Intestinal Obstruction
Abstract
Background: Gastrointestinal tract is the most common site for NETs. After the appendix, small bowel is the second most common site affected. Intestinal NETs are commonly asymptomatic. 70-80% of intestinal carcinoids are asymptomatic and found incidentally at the time of suregry. In literature very few cases of intestinal NETs present as acute intestinal obstruction. Usually they have an indolent, intermittent, or subacute onset with non specific bowel symptoms. So misdiagnosis is common in view of vague symptoms and most cases are treated as irritable bowel syndrome.
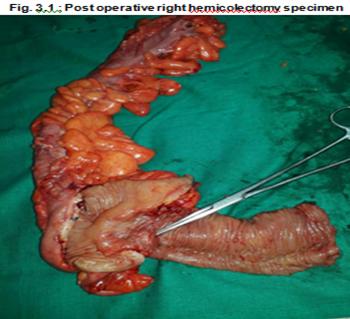
Case Presentation : 42 year old female presented with complaints of diffuse abdominal pain and obstipation for 2 days. She also had history of vomiting 2 episodes. No other significant history. On general examination patient was dehydrated with tachycardia. On abdomen examination, there was guarding in the right iliac fossa, hypogastrium and left iliac fossa. Bowel sounds were sluggish. Per rectal examination was normal. Abdomen x ray erect showed multiple air fluid levels. CECT abdomen showed dilated, fluid filled small bowel of diameter 3.2 cm with multiple air fluid levels suggesting small bowel obstruction. It also showed evidence of fat density lesion of size 3 cm noted arising from small bowel loop. Emergency laparotomy was done. Small bowel was dilated from duodeno-jejunal flexure to ileocaecal junction. Large bowel was found to be collapsed.At terminal ileum, 2 cm. proximal to ileocaecal junction a 3*2 cm irregular mass was palpable. A complex cyst of size 3*3 cm was found in the right ovary. Right hemiclectomy with ileotransverse anastomosis along with right oopherectomy was done. HPE report was well differentiated neuroendocrine tumour grade 1 with mature cystic teratoma of right ovary.
Conclusion : Till now only few cases of NET presenting as acute obstruction have been reported in literature. Carcinoid tumors are rare tumors of the Gastro intestinal tract, however, are the most common primary tumors of the small intestine. Most of these tumors have a very indolent course and may present with non specific symptoms. However in this case intestinal NET presents as acute intestinal obstruction
Keywords: Neuro endocrine tumor, acute intestinal obstruction, Right hemicolectomyFull Text:
PDFReferences
Singhal H. Carcinoid tumor, Intestinal. http://www. emedicine.com.
Burke AP, Thomas RM, Elsayed AM, Sobin LH. Carcinoids of the jejunum and ileum: an immunohistochemical and clinicopathologic study of 167 cases. Cancer. 1997;79: 1086–1093.
Marshall JB, Bodnarchuk G. Carcinoid tumors of the gut. Our experience over three decades and review of the literature. J Clin Gastroenterol. 1993;16(2): 123–9.
Eriksson B, Klopel G, Krenning E. Consensus guidelines for the management of patients with digestive neuroendocrine tumors well-differentiated jejuno-ileal tumor/carcinoma. Neuroendocrinology. 2008;87:8–19
Oberndorfer S. Karzinoide tumoren des dünndarms. Frankfurt Zietschrif fur Pathologie. 1907;1:426–429.
Broaddus RR, Herzog CE, Hicks MJ. Neuroendocrine tumors (carcinoid and neuroendocrine carcinoma) presenting at extra-appendiceal sites in childhood and adolescence. Arch Pathol Lab Med. 2003;127(9):1200–3.
Strodel WE, Vinik AI, Thompson NW. In: Endocrine Surgery Update. Thompson NW, Vinik AI, editor. New York, NY: Grune and Stratton; 1983. Small bowel carcinoid tumors and the carcinoid syndrome; pp. 277–291.
Levy AD, Sobin LH. Gastrointestinal Carcinoids: Imaging features with clinicopathologic comparison Raddiographics 2007:27(1)237-257
Basson MD, Ahlman H, Wangberg B. Biology and management of the midgut carcinoid. Am J Surgery. 1993;165: 288–297.
Oberg K, Stridsberg M. Chromogranins as diagnostic and prognostic markers in neuroendocrine tumours. Advances in experimental medicine and biology. 2000;482:329–337.
Ramage JK, Davies AH. Guidelines for the management of gastroenteropancreatic neuroendocrine tumours. Gut. 2004;54 Suppl 4:iv1–iv16.[PMC free article]
Que FG, Nagorney DM. Hepatic resection for metastatic neuroendocrine carcinomas. American Journal of Surgery. 1995;169:36–42.
Chen H, Hardacre JM. Isolated liver metastases from neuroendocrine tumors: does resection prolong survival? Journal of the American College of Surgeons. 1998;187: 88–92.
Chamberlain RS, Canes D. Hepatic neuroendocrine metastases: does intervention alter outcomes? Journal of the American College of Surgeons. 2000;4:432–445.
Janson ET, Holmberg L. Carcinoid tumors: Analysis of prognostic factors and survival in 301 patients from a referral center. Annals of Oncology. 1997;8:685–690.
Refbacks
- There are currently no refbacks.

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
An Initiative of The Tamil Nadu Dr MGR Medical University