Epidemiological and clinical characteristics of Talaromyces marneffei infection: A case series from a tertiary care hospital in South India.
Abstract
Introduction: Talaromyces marneffei, previously known as Penicillium marneffei is a dimorphic fungi mainly affecting immunocompromised individuals and is endemic in North-Eastern regions of India. It is the third most common infection among individuals infected with acquired immunodeficiency syndrome (AIDS). It is acquired by inhalation of conidia. After an initial respiratory infection, it can disseminate. We are describing here the different spectrum of talaromycosis, as seen in our centre.
Methods: Fourpatients who hadlaboratory confirmed diagnosis of Talaromyces marneffei infection, presenting to Christian Medical College, Vellore over a period of 4 years are included.
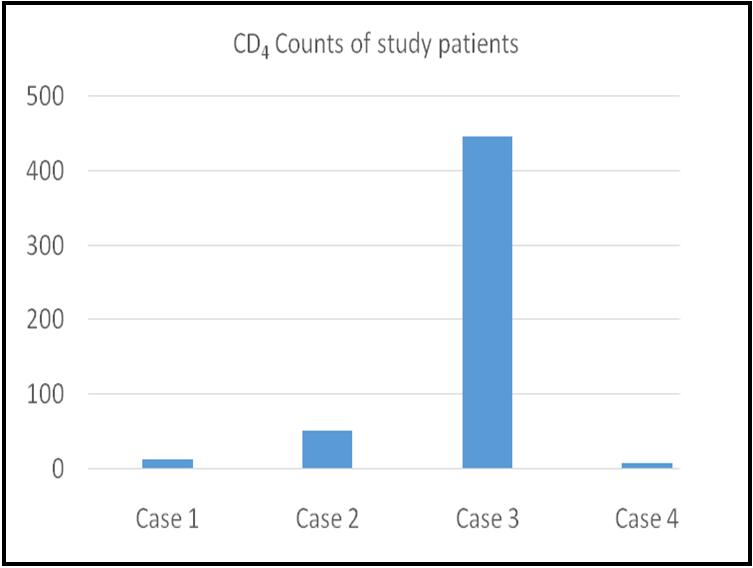
Results & Discussion: Threepatients (75%) were from the North-Eastern regions of India, with the remaining one hailing from Bangladesh. All patients were immunosuppressed with AIDS being the predominant underlying cause (in 3 patients). CD4 counts of the patients ranged from 7-50 cells/µl. One patient was co-infected with human immunodeficiency virus (HIV) and hepatitis B virus.The clinical presentations of the patients ranged from generalised weakness, multifocal osteomyelitis, papular skin eruption or fever with necrotic nodules over skin. T. marneffei was isolated from bone marrow of first patient, skin biopsy of second and T10 vertebral tissue of the third patient. The organism was cultured from bothbone marrow and skin biopsy from the fourth patient, suggesting dissemination. Three out of 4 patients (75%) survived aftertreatment with amphotericin B and itraconazole. However, one patient succumbed to the infection.
Conclusion: Talaromycosis is endemic in North-Eastern regions of India but with increased medical tourism, there is need for awareness of varying clinical presentations of thisdisease. This will aid in early diagnosis and appropriate management of these immunocompromised patients.
Full Text:
PDFReferences
. Samson RA, Yilmaz N, Houbraken J, Spierenburg H, Seifert KA, Peterson SW, et al. Phylogeny and nomenclature of the genus Talaromyces and taxa accommodated in Penicillium subgenus Biverticillium. Stud Mycol. 2011 Nov 15;70(1):159–83.
. Segretain G. Penicillium Marneffei N. Sp., Agent D’une Mycose Du Système Réticulo-Endothélial. Mycopathol Mycol Appl. 1959 Nov 1;11(4):327–53.
Sirisanthana T, Supparatpinyo K. Epidemiology and management of penicilliosis in human immunodeficiency virus-infected patients. Int J Infect Dis. 1998 Jul 1;3(1):48–53.
Nierman WC, Fedorova-Abrams ND, Andria nopoulos A. Genome Sequence of the AIDS-Associated Pathogen Penicillium marneffei (ATCC18224) and Its Near Taxonomic Relative Talaromyces stipitatus (ATCC10500). Genome Announc [Internet]. 2015 Feb 12;3(1). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4333666/
Cooper CR, McGinnis MR. Pathology of Penicillium marneffei. An emerging acquired immunodeficiency syndrome-related pathogen. Arch Pathol Lab Med. 1997 Aug;121(8):798–804.
Deng Z, Ribas JL, Gibson DW, Connor DH. Infections caused by Penicillium marneffei in China and Southeast Asia: review of eighteen published cases and report of four more Chinese cases. Rev Infect Dis. 1988 Jun;10(3):640–52.
Jayanetra P, Nitiyanant P, Ajello L, Padhye AA, Lolekha S, Atichartakarn V, et al. Penicilliosis marneffei in Thailand: report of five human cases. Am J Trop Med Hyg. 1984 Jul;33(4):637–44.
Vyawahare CR, Misra RN, Gandham NR, Angadi KM, Paul R. Pencillium keratitis in an Immunocompetent Patient from Pune, Maharashtra, India. J Clin Diagn Res JCDR. 2014 Jul;8(7):DD01-02.
Anutarapongpan O, Thanathanee O, Suwan-Apichon O. Penicillium keratitis in a HIV-infected patient. BMJ Case Rep. 2016 Aug 17;2016.
Supparatpinyo K, Khamwan C, Baosoung V, Nelson KE, Sirisanthana T. Disseminated Penicillium marneffei infection in southeast Asia. Lancet Lond Engl. 1994 Jul 9;344(8915):110–3.
Piehl MR, Kaplan RL, Haber MH. Disseminated penicilliosis in a patient with acquired immunodeficiency syndrome. Arch Pathol Lab Med. 1988 Dec;112(12):1262–4.
Vanittanakom N, Cooper CR, Fisher MC, Sirisanthana T. Penicillium marneffei Infection and Recent Advances in the Epidemiology and Molecular Biology Aspects. Clin Microbiol Rev. 2006 Jan;19(1) :95–110.
Singh PN, Ranjana K, Singh YI, Singh KP, Sharma SS, Kulachandra M, et al. Indigenous Disseminated Penicillium marneffei Infection in the State of Manipur, India: Report of Four Autochthonous Cases. J Clin Microbiol. 1999 Aug;37(8):2699–702.
Michael JS, Abraham OC, Mathai D, Mathews MS. Varied clinical manifestations of Penicillium marneffei in patients with human immunodeficiency virus: a report from south India. Mycoses. 2005 Mar;48(2):120–1.
Chan JF, Lau SK, Yuen K-Y, Woo PC. Talaromyces (Penicillium) marneffei infection in non-HIV-infected patients. Emerg Microbes Infect. 2016 Mar;5(3):e19.
De Monte A, Risso K, Normand A-C, Boyer G, L’Ollivier C, Marty P, et al. Chronic pulmonary penicilliosis due to Penicillium marneffei: late presentation in a french traveler. J Travel Med. 2014 Aug;21(4): 292–4.
Refbacks
- There are currently no refbacks.

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
An initiative of The Tamil Nadu Dr M.G.R. Medical University