Tumour excision and hip morphology correction in multiple hereditary exostoses by ganz safe surgical dislocation-A case report
Abstract
Multiple hereditary exostoses also known as diaphyseal aclasias,
most common benign bone disorder in children, is an autosomal dominant genetic disorder with
complete penetrance, with an incidence of 150,000 individuals commonly occurring along the
metaphysis of the long bones. Proximal femur is affected approximately 90 of individuals associated
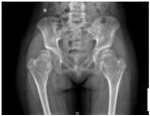
with growth disturbance, acetabular dysplasia and possible subluxation.Case We present a case of
14 year old girl who had come with complaints of multiple painless swellings involving her joints, with
a similar family history. Clinico-radiologically she was diagnosed with multiple hereditary exostoses.
Patient had difficulty in walking for a longer duration, squatting, sitting crossed leg intraarticular
exostosis of proximal femur was treated by excision osteotomy and ganz safe surgical
dislocation.Discussion Hereditary exostosis is an intriguing genetic condition with a clinical impact in
the field of orthopaedics. The abnormal chondro- osseous growths are a consequence of dysplasia in
the peripheral part of growth plate. In the particular case we opted to perform excision osteotomy of
proximal femur and ganz method of safe surgical dislocation in order to improve the range of
movements, relieve pain around the hip joint. postoperatively, there was a definitive improvement in
range of motion but there was no obvious deformity correction, as there was no gross alteration in the
biomechanics of the hip joint.Conclusion Despite complete excision of the exostosis mass followed by
a safe surgical dislocation, the hip was still abnormal though there was improvement in the range of
motion around the hip. Hence concluding that ganz method of surgical dislocation alone is insufficient
to correct hip morphology in a case of MHE, as it further requires a varus osteotomy of the proximal
femur to restore the normal biomechanics of the hip joint.
Full Text:
PDFReferences
Judith et al. Review on multiple osteochondromas. Orphanet journal of rare diseases. 2008;3(3): .
Heleenstael.M, Annemare, L. Skeletal maturity of children with multiple osteochondroma :is
diminished stature due to a systemic influence. Jchildorthop. 2015;9(3): 397-40
Jonathan streber, R, John dorman, P. Manifestations of hereditary multiple exostoses. Journal of
American Academy of orthopod surgery. 2005;13(1): 110-120.
Malgon, V. Development of hip dysplasia in hereditary multiple exostoses. J.paediatrorthop. 2001;
(1): 205-211.
Noonan, K.J, Feinberg, J.R, Snead, J, Wuitz, L.D. Natural history of multiple hereditary
osteochondromatosis of the lower extremity and Ankle. J.paediatr orthop. 2002;22(1): 120-124.
Francannet et al. Genotype- phenotype correlation in hereditary multiple exostoses. J Med genet.
;38(1): 430-434.
Black, B, Dooley, J, Pyper, A, Reed, M. Multiple hereditary exostoses: Anepidemiologic study of an
isolated community in Manitoba. J clinic orthop. 1983;287(15): 212-217.
Solomon, L. Bone growth in diaphysealaclasias. JBJS. 1961;43(2): 700-716.
Nawata, K, Teshima, R, Minamizaki, T, Yamamoto, K. Knee deformities in multiple hereditary
exostoses:Alongiitudinal radiographic study. ClinorthopRelat Res. 1995;313(2): 194-199.
Felix, N.A, Mazur, J.M, Lovelest, E.A. Acetabular dysplasia associated wtih hereditary multiple
exostoses: Acase report. JBJS. 2000;82(1): 555-557.
. Asim makhdom et al, M. Hip joint osteochondroma: systematic review of the literature and report
of three further cases. J of advanced orthopaedics. 2014;32(2): 52-55
Refbacks
- There are currently no refbacks.

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
An initiative of The Tamil Nadu Dr M.G.R. Medical University