 University Journal of Surgery and Surgical Specialities
University Journal of Surgery and Surgical Specialities
Transoral Transpharyngeal approach to Craniovertebral Junction: Indications, Management and outcomes in a Survey of 7 Cases
Abstract
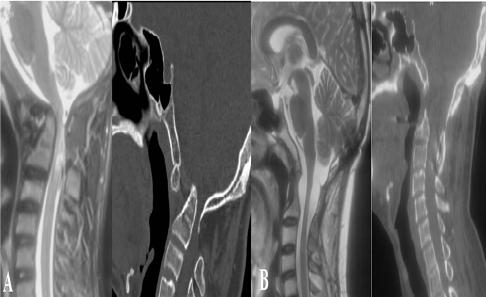
Introduction: The transoral-transpharyngeal surgical
approach is a direct operative approach for pathology
ventral to the craniovertebral junction and upper spinal
cord. In selected patients, this approach is effective in the
treatment of extradural compressive lesions
from the cervico-medullary junction to the C3 vertebra. We
present 7 patients who underwent transoral
transpharyngeal surgeries by a single surgeon (BVJ) for
ventral CVJ compression due to different pathologies.
Material and Methods: Retrospective data analysis of
7 patients who underwent transoral transpharyngeal
surgeries for various pathologies affecting the
craniovertebral junction was performed from January 2015
to January 2017. The hospital records, outpatient
physician records, and radiographic studies of all
7 patients were reviewed. Results: The mean age of the
study group was 36 (range 10-64) years. There were
4 (57.1%) males and 3 (42.9%) females. 6 (85.7%) out of
seven patients presented with features of cervical cord
compression. In one patient (14.3%) only neck pain with
restriction of neck movement was present. Of the
7 patients, 3 (42.8%) had irreducible atlantoaxial
dislocation with basilar invagination, 2 (28.6%) had
irreducible atlantoaxial dislocation and 2 (28.6%) had CVJ
tuberculosis. The most common presenting symptom of
the group was spastic quadriparesis and paresthesias
involving all four limbs. The mean preoperative Nurick
grade was 1.9 and the mean imJOA score was 13.5/19 for
the group. All patients were operated through
transoral-transpharyngeal approach and all of them
underwent occipito-cervical fusion subsequently. 5 (71.4%)
out of 7 patients had symptomatic improvement
postoperatively. One patient (14.3%) required
tracheostomy postoperatively for prolonged ventilation and
he was discharged on BIPAP.
However he expired after three months of surgery due
ventilator associated pneumonia. One patient (14.3%) had
transient hoarseness of voice and difficulty in swallowing
postoperatively for which improved over next two weeks. The
mean follow-up of our series (n=5) was 18.4 months. One
patient was lost to follow-up. The mean Nurick grade
improved to 0 and mean imJOA improved to 19/19 at
follow-up. All patients were symptom-free at follow-up and
there was radiological reduction with bony fusion in all of
them. Conclusion: Transoral odontoidectomy is a safe and
efficacious approach for the treatment of selected patients
with compressive pathology of the ventral brain stem and
upper cervical cord. Patients must be selected judiciously and
a detailed radiological examination is advised to define the
extent of compression, reducibility, and instability present in
an individual patient.
Full Text:
PDFReferences
Crockard AH, Sen CN. The transoral approach for the
management of intradural lesions at the craniovertebral
junction: review of 7 cases. Neurosurgery 1991;28:88–98.
Hadley MN, Spetzler RF, Sonntag VK. The transoral
approach to the superior cervical spine: a review of 53 cases
of extradural cervicomedullary compression. J Neurosurg
;71:16–23.
Arunkumar MJ, Rajshekhar V. Outcome in neurologically
impaired patients with craniovertebral junction tuberculosis:
results of combined anteroposterior surgery. J Neurosurg
Spine 2002;97:166–71.
Crockard HA, Pozo JL, Ransford AO, Stevens JM, Kendall
BE, Essigman WK. Transoral decompression and posterior
fusion for rheumatoid atlanto-axial subluxation. Bone Jt J
;68:350–6.
Di Lorenzo N. Transoral approach to extradural lesions of
the lower clivus and upper cervical spine: an experience of
cases. Neurosurgery 1989;24:37–42.
Kanavel AB. Bullet located between the atlas and the base
of the skull: technique of removal through the mouth. Surg
Clin Chic 1917;1:9.
Mullan S, Naunton R, Hekmat-Panah J, Vailati G. The use
of an anterior approach to ventrally placed tumors in the
foramen magnum and vertebral column. J Neurosurg
;24:536–43.
Menezes AH, VanGilder JC. Transoral-transpharyngeal
approach to the anterior craniocervical junction: ten-year
experience with 72 patients. J Neurosurg 1988;69:895–903.
Jain VK, Behari S, Banerji D, Bhargava V, Chhabra DK.
Transoral decompression for craniovertebral osseous
anomalies: perioperative management dilemmas. Neurol
India 1999;47:188.
Welch WC, Kassam A. Endoscopically assisted
transoral-transpharyngeal approach to the craniovertebral
junction. Neurosurgery 2003;52:1511–2.
Pollack IF, Welch W, Jacobs GB, Janecka IP. Frameless
Stereotactic Guidance: An Intraoperative Adjunct in the
Transoral Approach for Ventral Cervicomedullary Junction
Decompression. Spine 1995;20:216–20.
Gehweiler Jr JA, Daffner RH, Roberts Jr L.
Malformations of the atlas vertebra simulating the Jefferson
fracture. Am J Roentgenol 1983;140:1083–6.
Menezes AH, VanGilder JC, Graf CJ, McDonnell DE.
Craniocervical abnormalities: a comprehensive surgical
approach. J Neurosurg 1980;53:444–55.
Menezes AH, VanGilder JC. Transoral-transpharyngeal
approach to the anterior craniocervical junction: ten-year
experience with 72 patients. J Neurosurg 1988;69:895–903.
Menezes AH. Surgical approaches: postoperative care
and complications “transoral–transpalatopharyngeal
approach to the craniocervical junction.” Childs Nerv Syst
;24:1187–93.
Hadley MN, Spetzler RF, Sonntag VK. The transoral
approach to the superior cervical spine: a review of 53 cases
of extradural cervicomedullary compression. J Neurosurg
;71:16–23.
Refbacks
- There are currently no refbacks.

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
An Initiative of The Tamil Nadu Dr MGR Medical University