A Case Report on Anaesthetic Management of Ruptured Abdominal Aortic Aneurysm
Abstract
Ruptured abdominal aortic aneurysm is commonly fatal with 75% mortality rate the most common cause being atherosclerosis1. Intraperitoneal rupture invariably leads to cardiovascular collapse and death. Emergency surgery for abdominal aortic aneurysm carries a high mortality rate of 90%.2 Even patients who survive the initial procedure are at high risk of complications like renal, cardiac, hematological, respiratory or gastrointestinal failure.
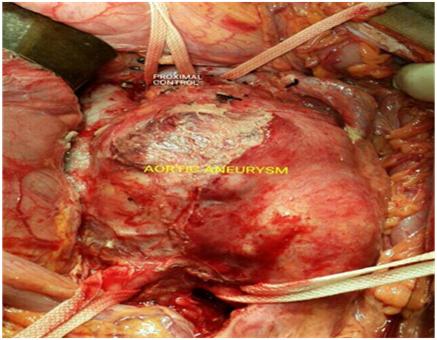
We report a case of 59 years old male who was diagnosed with ruptured abdominal aortic aneurysm. Contrast CT of abdomen was suggestive of ruptured abdominal aortic aneurysm below the level of renal arteries extending up to the level of bifurcation of aorta. He underwent abdominal aortic aneurysm repair under ASA PS IV E. Patient was monitored intraoperatively with invasive blood pressure monitoring, ETCO2, CVP, temperature, SPO2. Hemodynamic changes during clamping and unclamping was effectively managed using nitroglycerine and Dopamine infusion. The duration of full cross clamping was 40 minutes and partial cross clamping time was 55 minutes.Patient was maintained hemodynamically stable throughout the procedure with intensive monitoring. In the Post operative period the patient was hemodynamically stable and urine output was within normal limits. Post operative period was uneventful and patient was discharged after 15 days. With effective anaesthetic management the patient survived without developing any complications.
Full Text:
PDFReferences
Wylie and churchill davidson’s A practice of anaesthesia 7th edition
Miller’s anaesthesia eighth edition
Hirsch AT, Haskal ZJ, Hertzer NR et al. ACC/AHA 2005 Practice Guidelines for the management of Patients with peripheral arterial disease. Circulation 2006;113(11):e463- 654
Patterson BO, Holt , Hinchliffe R, Loftus I M, Thompson MM. Predicting the risk in elective Abdominal aortic aneurysm repair: a systematic review of current evidence, Eur J Endovascular Surg, 2008, vol. 36 (p 637-45)
Grant , Grayson AD, Mitchell , McCollum CN. Evaluation of five risk prediction models for elective abdominal aortic aneurysm repair using the UK National Vascular Database, Br J Surg , 2012, vol. 99 (p 673-9)
Brewster DC, Cronenwett, Hallett JW, Johnson KW, Krupski WC, Matsumura JS. Guidelines for the treatment of abdominal aortic aneurysms, J Vasc Surg , 2003, vol. 37 (p 1106-17)
Chaikof EL, Brewster DC, Dalman RL, et al. The care of patients with an abdominal aortic aneurysm: the Society for Vascular Surgery practice guidelines, J Vasc Surg, 2009, vol. 50 (pS2-49)
2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, Davila-Roman VG, Gerhard-Herman MD, Holly TA, Kane GC, Marine JE, Nelson MT, Spencer CC, Thompson A, Ting HH, Uretsky BF, Wijeysundera DN.Epub 2014 Aug 1.
Refbacks
- There are currently no refbacks.

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
An initiative of The Tamil Nadu Dr M.G.R. Medical University