A novel, safe and effective chelating regimen for treatment of Lead toxicity
Abstract
Introduction
Lead toxicity is a recognized occupational hazard with long term morbidity and mortality. Still, treatment guidelines regarding choice and doses of chelating agents are not standardised1. We present a novel and safe low dose intermittent regimen of calcium disodium EDTA2 (CaNa2EDTA) used for treating patients with lead toxicity.
Discussion
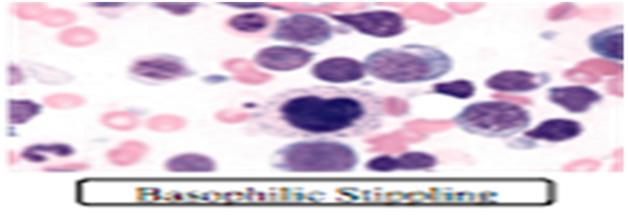
A 40 years male, battery factory worker presented with abdominal cramps, diarrhoea, weight loss, irritability, fine tremors and microcytic hypochromic anaemia nresponsive to iron supplements for two years. Tests showed haemoglobin 7.8 gm/dl, MCV 75.0 fl with Erythrocyte morphology showing classical basophilic stippling. His serum blood levels were 182.3 ug/dl (Normal: <5ug/dl). Another 23 years old male, painter, with subacute progressive quadriparesis and iron unresponsive microcytic hypochromic anaemia, had blood lead levels 52.3 ug/dl and was diagnosed to have lead neuropathy. Both the patients received helation with a novel regimen consisting of low dose (1 gm) CaNa2EDTA given once a week for eight weeks followed by maintenance with d-penicillamine. to non-toxic range in 20 weeks.The first patient showed clinical improvement with initial two doses of CaNa2EDTA and blood lead levels reduced to non-toxic range within 24 weeks. The second patient showed gradual neurological improvement in motor power over 30 weeks with pursuance of functional activities of daily living and blood lead levels reducedto non-toxic range in 20 weeks.CaNa2EDTA is usually recommended in a dosage of 50–80 mg/kg/day for 2–5 days, requiring maintenance of hydration, electrolyte monitoring to avoid nephrotoxicity.However, we used a low dose (20 mg/kg) intermittent dosing regimen of CaNa2EDTA which in addition to avoiding nephrotoxicity, also prevented rebound elevation of blood lead due to resorption from the bones.
Full Text:
PDFReferences
Kianoush S, Sadeghi M, Balali-Mood M. Recent Advances in the Clinical Management of Lead Poisoning. Acta Med Iran. 2015;53(6):327–36.
IARC monographs on the evaluation of carcinogenic risks to humans volume 87: Inorganic and organic lead compounds. International Agency for Research on Cancer, 2004. http://monographs.iarc.fr/ENG/Monographs/vol87/mono87.pdf.
Chandran L, Cataldo R. Lead poisoning: basics and new developments. Pediatr Rev 2010;31(10):399-405.
Deaths associated with hypocalcemia from chelation therapy: Texas, Pennsylvania and Oregon, 2003-2005. Mortality and Morbidity Weekly Report March 3, 2006. 55(08); 204-207.
Bradberry S, Vale A. A comparison of sodium calcium edetate (edetate calcium disodium) and succimer (DMSA) in the treatment of inorganic lead poisoning.ClinToxicol (Phila).2009 Nov;47(9):841–58
.6. Mikirova, Nina, et al. "EDTA chelation therapy in the treatment of toxic metals exposure." Spatula DD-Peer Reviewed Journal on Complementary Medicine and Drug Discovery 1.2 (2011): 81-89.
Gracia RC, Snodgrass WR. Lead toxicity and chelation therapy. Am J Health Syst Pharm. 2007 Jan 1;64(1):45–53.
Flora SJS, Pachauri V. Chelation in metal intoxication. Int J Environ Res Public Health. 2010 Jul;7(7):2745–88.
Bradberry S, Vale A. Dimercaptosuccinic acid (succimer; DMSA) in inorganicleadpoisoning. ClinicalToxicology. 2009 Aug 1;47(7):617–31.
Refbacks
- There are currently no refbacks.

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
An initiative of The Tamil Nadu Dr M.G.R. Medical University