A SYSTEMIC DISEASE WITH GI PRESENTATION - A CASE REPORT
Abstract
Apart from the many disorders that affect the GI tract primarily like
achalsia , carcinomas infections, inflammatory bowel disease and so on the GI tract can be
prominently involved in a host of systemic disorders like connective tissue disorders, scleroderma,
henoch scholein purpura ,HIV, carcinoids etc. The early identification of these also aid in the
diagnosis and subsequently leading on to appropriate treatment which may lead to substantial
reduction in both morbidity and mortality as in our case below.CASE REPORT A 63 years old male
presented with a 6 months history of early satiety, malaise, easy fatigability and significant weight
loss. On examination he was found to be pale with generalised lymphadenopathy and
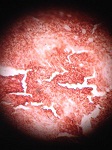
hepatosplenomegaly. Upper and lower GI endoscopies were done which showed nodular lesions
which were biopsied sent for HPE which showed small round cells with central nucleus and a rim of
cytoplasm but was inconclusive. Imaging studies were done which showed a greatly thickened gastric
wall, sigmoid colon and rectum along with free fluid in both peritoneal and pleural cavities. In view of
the lyphadenopathy suggesting a systemic aetiology it was excised and sent for HPE which showed
enlarged follicles with germinal centres and was suggested further staining studies. The slides were
sent for immunohistochemistry with CD 20 which turned out highly positive thus confirming the
diagnosis of NON HODGKINS LYMPHOMA. A peripheral smear was done which also supported the
diagnosis showing 85 blast cells suggesting a AML-M2 type blast transformation of the NHL. He was
subsequently referred to the oncology department where he was started on R-CHOP regimen
chemotherapy along with further sub typing follow up of NHL.
achalsia , carcinomas infections, inflammatory bowel disease and so on the GI tract can be
prominently involved in a host of systemic disorders like connective tissue disorders, scleroderma,
henoch scholein purpura ,HIV, carcinoids etc. The early identification of these also aid in the
diagnosis and subsequently leading on to appropriate treatment which may lead to substantial
reduction in both morbidity and mortality as in our case below.CASE REPORT A 63 years old male
presented with a 6 months history of early satiety, malaise, easy fatigability and significant weight
loss. On examination he was found to be pale with generalised lymphadenopathy and
hepatosplenomegaly. Upper and lower GI endoscopies were done which showed nodular lesions
which were biopsied sent for HPE which showed small round cells with central nucleus and a rim of
cytoplasm but was inconclusive. Imaging studies were done which showed a greatly thickened gastric
wall, sigmoid colon and rectum along with free fluid in both peritoneal and pleural cavities. In view of
the lyphadenopathy suggesting a systemic aetiology it was excised and sent for HPE which showed
enlarged follicles with germinal centres and was suggested further staining studies. The slides were
sent for immunohistochemistry with CD 20 which turned out highly positive thus confirming the
diagnosis of NON HODGKINS LYMPHOMA. A peripheral smear was done which also supported the
diagnosis showing 85 blast cells suggesting a AML-M2 type blast transformation of the NHL. He was
subsequently referred to the oncology department where he was started on R-CHOP regimen
chemotherapy along with further sub typing follow up of NHL.
Full Text:
PDFReferences
DAWSON IM, CORNES primary malignant lymphoid tumours of the intestinal tract Br j surgery
Lewin KJ lymphomas of GIT cancer 1978
Loehr et al primary lymphoma of GI 100 cases review
Ehrilch an Sherlock p gastrointestinal manifestations of malignant lymphoma gastroenterology
Koch German study j clinical oncology 2001
Papaxonisis g et al 128 cases in Greece primary NHL gi tract leuk lymphoma 2006 47:2140
Refbacks
- There are currently no refbacks.

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
An initiative of The Tamil Nadu Dr M.G.R. Medical University